A Systematic Review of Sexual Minority Women’s Experiences of Health Care in the UK


Abstract
1. Background
2. Methods
2.1. Searches
2.2. Study Selection, Data Extraction, Quality Assessment
2.3. Synthesis Methods
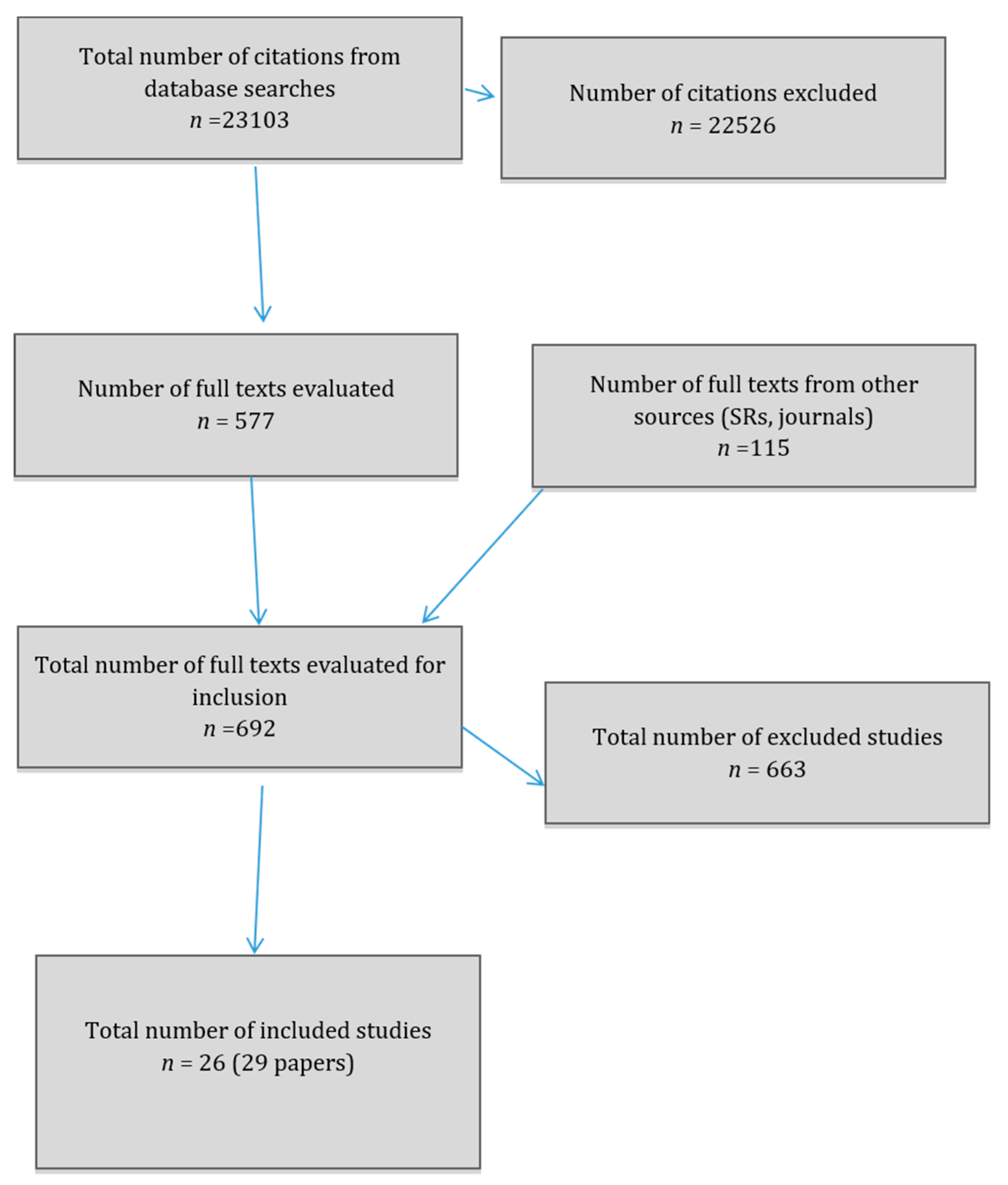
3. Results
3.1. Qualitative Study Results
3.1.1. Unhelpful Health Ambience
3.1.2. Assumed Heterosexuality/Heteronormativity
3.1.3. Being “Out” or Not
3.1.4. Responses to Being Out
3.1.5. Ignorance
3.1.6. Impact on Sexual Minority Women
3.1.7. Challenging/Complaining
3.1.8. Bisexual and Trans Participants
3.2. Quantitative Comparative Results
3.3. General Experience of Health from Non-Comparative Studies
4. Discussion
4.1. Summary of Findings
4.2. Strengths and Weaknesses of the Systematic Review
4.3. Comparison to Previous Research
5. Implications and Recommendations for Practitioners
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Blondeel, K.; Say, L.; Chou, D.; Toskin, I.; Khosla, R.; Scolaro, E.; Temmerman, M. Evidence and knowledge gaps on the disease burden in sexual and gender minorities: A review of systematic reviews. Int. J. Equity Health 2016, 15, 16. [Google Scholar] [CrossRef]
- Edmondson, D.; Hodges, R.; Williams, H. The Lesbian, Gay, Bisexual and Trans Public Health Outcomes Framework Companion Document; updated; National LGB&T Partnership: London, UK, 2016. [Google Scholar]
- Hudson-Sharp, N.; Metcalf, H. Inequality among Lesbian, Gay Bisexual and Transgender Groups in the UK: A Review of Evidence; National Institute of Economic and Social Research: London, UK, 2016. [Google Scholar]
- Meads, C.; Pennant, M.; McManus, J.; Bayliss, S. A Systematic Review of Lesbian, Gay, Bisexual and Transgender Health in the West Midlands Region of the UK Compared to Published UK Research; University of Birmingham: Birmingham, UK, 2011; Available online: http://www.birmingham.ac.uk/Documents/collegemds/haps/projects/WMHTAC/REPreports/2009/LGBThealth030409finalversion.pdf (accessed on 26 January 2011).
- Semlyen, J.; King, M.; Varney, J.; Hagger-Johnson, G. Sexual orientation and symptoms of common mental disorder or low wellbeing: Combined meta-analysis of 12 UK population health surveys. BMC Psychiatry 2016, 16, 67. [Google Scholar] [CrossRef] [PubMed]
- Saunders, C.L.; Mendonca, S.; Lyratzopoulos, Y.; Abel, G.A.; Meads, C. Associations between sexual orientation, and overall and site-specific diagnosis of cancer: Evidence from two national patient surveys in England. J. Clin. Oncol. 2017, 35, 3654–3661. [Google Scholar] [CrossRef]
- Robinson, C.; Galloway, K.Y.; Bewley, S.; Meads, C. Lesbian and bisexual women’s gynaecological conditions: A systematic review. BJOG 2017, 124, 381–392. [Google Scholar] [CrossRef]
- Hodson, K.; Meads, C.; Bewley, S. Lesbian and bisexual women’s likelihood of becoming pregnant: A systematic review. BJOG 2017, 124, 393–402. [Google Scholar] [CrossRef]
- Meads, C.; Moore, D. Breast cancer in lesbians and bisexual women: Systematic review of incidence, prevalence and risk studies. BMC Public Health 2013, 13, 1127. [Google Scholar] [CrossRef]
- Shahab, L.; Brown, J.; Hagger-Johnson, G.; Michie, S.; Semlyen, J.; West, R.; Meads, C. Sexual orientation identity and tobacco and hazardous alcohol use: Findings from a cross-sectional English population survey. BMJ Open 2017, 7, e015058. [Google Scholar] [CrossRef] [PubMed]
- Williams, H.; Varney, J.; Taylor, J.; Fish, J.; Durr, P.; Elan-Cane, C. The Lesbian, Gay, Bisexual and Trans Public Health Outcomes Framework Companion Document; Lesbian and Gay Foundation: Manchester, UK, 2013. [Google Scholar]
- Coulter, R.W.; Kenst, K.S.; Bowen, D.J.; Scout. Research funded by the National Institutes of Health on the health of lesbian, gay, bisexual and transgender populations. Am. J. Public Health 2014, 104, e105–e112. [Google Scholar] [CrossRef]
- St. Pierre, M. Under what conditions do lesbians disclose their sexual orientation to primary healthcare providers? A review of the literature. J. Lesbian Stu. 2012, 16, 199–219. [Google Scholar] [CrossRef]
- Dahl, B.; Fylkesnes, A.M.; Sørlie, V.; Malterud, K. Lesbian women’s experiences with healthcare providers in the birthing context: A meta-ethnography. Midwifery 2013, 29, 674–681. [Google Scholar] [CrossRef] [PubMed]
- Harding, R.; Epiphaniou, E.; Chidgey-Clark, J. Needs, experiences, and preferences of sexual minorities for end-of-life care and palliative care: A systematic review. J. Palliat. Med. 2012, 15, 602–611. [Google Scholar] [CrossRef] [PubMed]
- Harden, A. Mixed-Methods Systematic Reviews: Integrating Quantitative and Qualitative Findings; National Center for the Dissemination of disability Research (NCDDR): Washington, WA, USA, 2010. [Google Scholar]
- Lewin, S.; Bohren, M.; Rashidian, A.; Munthe-Kaas, H.; Glenton, C.; Colvin, C.J.; Garside, R.; Noyes, J.; Booth, A.; Tuncalpe, O.; et al. Applying GRADE-CERQual to qualitative evidence synthesis findings-paper 2: How to make an overall CERQual assessment of confidence and create a Summary of Qualitative Findings table. Implement Sci. 2018, 13, 10. [Google Scholar] [CrossRef] [PubMed]
- Guasp, A. Lesbian Gay and Bisexual People in Later Life; Stonewall: London, UK, 2011. [Google Scholar]
- Humphreys, S.; Worthington, V. Best Practice in Providing Healthcare to Lesbian, Bisexual and Other Women Who Have Sex with Women; National LGB&T Partnership: Manchester, UK, 2016. [Google Scholar]
- Light, B.; Ormandy, P.; Bottomley, R.; Emery, A. Lesbian, Gay & Bisexual Women in the North West: A Multi-Method Study of Cervical Screening Attitudes, Experiences and Uptake; University of Salford: Manchester, UK, 2011. [Google Scholar]
- Macredie, S. The Challenge for Change. Health needs of Lesbian, Gay and Bisexual People in Bradford and District; Equity Partnership: Bradford UK, 2010. [Google Scholar]
- River, L. Appropriate Treatment Older Lesbian, Gay and Bisexual People’s Experience of General Practice; Age of Diversity and Polari: London, UK, 2011. [Google Scholar]
- Balding, A. Young People in Cambridgeshire Schools, the Health-Related Behaviour Survey 2014, a Report for LGBT; The Schools Health Education Unit: Exeter, UK, 2014. [Google Scholar]
- Government Equalities Office (GEO). National LGBT Survey Research Report; UK Government Department for Education: Manchester, UK, 2018.
- Elliott, M.N.; Kanouse, D.E.; Burkhart, Q.; Abel, G.A.; Lyratzopoulos, G.; Beckett, M.K.; Schuster, M.A.; Roland, M. Sexual minorities in England have poorer health and worse health care experiences: A national survey. J. Gen. Intern. Med. 2014, 30, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.; Taylor, J.; Raitt, F. ‘It’s not me, it’s them’: How lesbian women make sense of negative experiences of maternity care: A hermeneutic study. J. Adv. Nurs. 2010, 67, 982–990. [Google Scholar] [CrossRef] [PubMed]
- Fish, J. Coming Out about Breast Cancer: Lesbian and Bisexual Women. Policy and Practice Implications for Cancer Services and Social Care Organisations; National Cancer Action Team and De Montfort University: Leicester, UK, 2010. [Google Scholar]
- Formby, E. Sex and relationships education, sexual health, and lesbian, gay and bisexual sexual cultures: Views from young people. Sex Educ. 2011, 11, 255–266. [Google Scholar] [CrossRef]
- Cherguit, J.; Burns, J.; Pettle, S.; Tasker, F. Lesbian co-mothers’ experiences of maternity healthcare services. J. Adv. Nurs. 2013, 69, 1269–1278. [Google Scholar] [CrossRef]
- Fenge, L.-A. Developing understanding of same-sex partner bereavement for older lesbian and gay people: Implications for social work practice. J. Gerontol. Soc. Work 2014, 57, 288–304. [Google Scholar] [CrossRef]
- Westwood, S. ‘We see it as being heterosexualised, being put into a care home’: Gender, sexuality and housing/care preferences among older LGB individuals in the UK. Health Soc. Care Community 2016, 24, e155–e163. [Google Scholar] [CrossRef] [PubMed]
- Carter, L.; Hedges, L.; Congdon, S. Using diversity interventions to increase cervical screening of lesbian and bisexual women. J. Psychol. Issues Organ. Cult. 2013, 3, 133–145. [Google Scholar] [CrossRef]
- Fish, J.; Williamson, I. Exploring lesbian, gay and bisexual patients’ accounts of their experiences of cancer care in the UK. Eur. J. Cancer Care 2018, 27. [Google Scholar] [CrossRef]
- Evans, M.; Barker, M. How do you see me? Coming out in counselling. Br. J. Guid. Counc. 2010, 38, 375–391. [Google Scholar] [CrossRef]
- Price, E. Coming out to care: Gay and lesbian carers’ experiences of dementia services. Health Soc. Care Community 2010, 18, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Somerville, C. Unhealthy Attitudes: The Treatment of LGBT People within Health and Social Care Services; Stonewall: London, UK, 2015. [Google Scholar]
- Willis, P.; Ward, N.; Fish, J. Searching for LGBT carers: Mapping a research agenda in social work and social care. Br. J. Soc. Work 2011, 41, 1304–1320. [Google Scholar] [CrossRef]
- Bristowe, K.; Hodson, M.; Wee, B.; Almack, K.; Johnson, K.; Daveson, B.A.; Koffman, J.; McEnhill, L.; Harding, R. Recommendations to reduce inequalities for LGBT people facing advanced illness: ACCESSCare national qualitative interview study. Palliat. Med. 2018, 32, 23–35. [Google Scholar] [CrossRef]
- McDermott, E.; Hughes, E.; Rawlins, V. Queer futures final report. Understanding Lesbian, Gay, Bisexual and Trans (LGBT) Adolescents’ Suicide, Self-Harm and Help-Seeking Behaviour; Department of Health Policy Research Programme: London, UK, 2016. [Google Scholar]
- Urwin, S.; Whittaker, W. Inequalities in family practitioner use by sexual orientation: Evidence from the English General Practice Patient Survey. BMJ Open 2016, 6, e011633. [Google Scholar] [CrossRef] [PubMed]
- Williams, H. Beyond Babies and Breast Cancer. Health Care Needs of Lesbian and Bisexual Women: An Overview of Available Evidence; The Lesbian & Gay Foundation: Manchester, UK, December 2013. [Google Scholar]
- McNair, R.; Hegarty, K. Guidelines for the Primary Care of Lesbian, Gay, and Bisexual People: A Systematic Review. Ann. Fam. Med. 2010, 8, 533–541. [Google Scholar] [CrossRef]
- Fish, J.; Evans, D.T. Promoting cultural competency in the nursing care of LGBT patients (Editorial). J. Res. Nurs. 2016, 21, 159–162. [Google Scholar] [CrossRef]


{kind=link}
| Study Author, Year | Study Design Method | Population, Setting | Number of Participants (Total Number in Study) | Recruitment | Sexual Orientation Ascertainment | Outcomes of Interest | Funding Publication Status |
|---|---|---|---|---|---|---|---|
| Almack et al. 2010 | Four focus groups | LGB community | 5 SMW (n = 15 total) | Unclear | Self-report | End of life care issues | Fully published, Funded by Burdett Trust for Nursing and Help the Aged (now Age UK) |
| Balding 2014 | Health-Related Behaviour Survey | School year 10—aged 14–15 | 1916 Cambridgeshire girls, of which 92 LGBT (n = 3918 total) | Through schools | Self-report LGB | GP practice issues | Grey literature report. Schools Health Education Unit. |
| Bristowe et al. 2018 | Semi-structured interviews | LGB community with advanced illnesses or their carers | 18 SMW (n = 40 total) | Through palliative care teams (three hospital, three hospice), and nationally through social/print media and LGBT community networks | Self-report LGB | Experience of receiving care when facing advanced illness | Fully published. Marie Curie Research Grant Scheme |
| Carter et al. 2013 | Individual and small group interviews | SMW in community | 5 SMW (n = 5 total) | Unclear | Self-report | Cervical screening issues | Fully published, funding unclear |
| Cherguit et al. 2013 | Semi-structured interviews | SMW in community | 10 lesbian mothers (n = 10 total) | Via a donor conception charity then snowball. | Self-report lesbian | Midwifery and delivery issues | Fully published, not funded |
| Elliot et al. 2014 | English General Practice Patient Survey 2009/10 | Women in community attending GPs | 1,021,541 women of which 0.6% lesbian, 0.5% bisexual. 86.1% heterosexual (n = 2,169,718 total) | Through GP surgeries | Self-report LGB using ONS categories | GP practice issues | Fully published, funded by UK Govt. Department of Health |
| Evans and Barker 2010 | Survey (open-ended questions) | Community | 47 women of which 44 SMW (n = 62 total) | Adverts including in Diva magazine | Self-report | Issues around mental health counselling | Fully published, funder unclear |
| Fenge 2014 | Semi-structured interviews at home or workplace. | Community | 1 lesbian (n = 4 total) | Snowball sample | Self-report | Bereavement experiences | Fully published, funding unclear |
| Fish 2010 | Semi-structured interviews | SMW in the community with breast cancer or had partner with breast cancer | 17 SMW (n = 17 total) | Flyers via networks, websites, email lists, LB women’s groups, cancer care services and Age Concern | Self-report | Breast cancer care experiences and issues | Grey literature, funded by National Cancer Action Team |
| Fish and Bewley 2010 | Survey (open ended questions) | SMW in the community | 5909 lesbian and bisexual women (n = 5909 total) | Promotional materials in gay and mainstream media and other distribution channels. | Self-report sexual minority | Nature of healthcare experiences, recommendations for improving services and any other healthcare experiences | Fully published, funded by Lloyds TSB Charitable Foundation |
| Fish and Williamson 2016 | Semi-structured interviews | LGB people in the community diagnosed with cancer in previous 5 years | 6 lesbians (n = 15 total) | Radio interviews, LGBT press articles, 50 local mainstream cancer groups, LGBT community-based groups, social media | Self-report LGB | Experiences of cancer care | Fully published, funded by Hope Against Cancer charity |
| Formby 2011 (and Formby 2011b) | Survey and focus groups | SMW in the community | 54 SMW (n = 54 total) | Online and through local press, LGBT networks and commercial gay scene | Self-report | Sexual health services | Fully published, funder unclear |
| GEO 2018 | Survey (online only) | LGBTI aged 16 or over | N women not given but approx. 45,402 (42%) (n = 108,100 total) | Via stakeholders, Pride events, national media, GEO, government social media, television interviews and online video | Self-report | Experiences of health services | Grey literature, funded by UK government |
| Guasp 2011 | Survey | Older LGB and heterosexual, community | N women unclear, n SMW unclear. (n = 2086 total) | Through YouGov panel supplemented with social media campaign | Unclear | Future care (other results not presented by gender) | Grey literature report. Funded by Stonewall |
| Humphreys et al. 2016 | Survey and 3 focus groups | SMW in the community | 101 women (n = 101 total) | Through National LGB&T Partnership social media | Self-report | Healthcare experiences | Grey literature, funding unclear |
| Ingham et al. 2016 | Semi-structured interviews | Older women in community | 8 women who had lost a same-sex partner (n = 8 total) | Adverts to relevant charities, support groups and services | Self-report partnership status | Bereavement experiences | Fully published, funding unclear |
| Knocker 2012 | Interviews | Older lesbians in community or sheltered housing | 4 lesbians (n = 8 total) | Unclear | Self-report | Experiences of health and social care | Grey literature report, funded by Joseph Rowntree Foundation |
| Lee et al. 2011 | Unstructured interviews | Lesbian mothers | 8 lesbians (n = 8 total) | Snowballing from first participant | Self-report | Positive and negative experiences of maternity care | Fully published, not funded |
| Light and Ormandy 2011 | Survey and 6 focus groups | Community | Survey 611 LGB women (n = 611 total), 60 in focus groups | Online survey, via Manchester Pride and Manchester Lesbian and Gay Foundation | Self-report | Cervical screening service experiences | Grey literature report, funded by NHS Cervical Screening Programme |
| Macredie 2010 | Survey, with open and closed questions | LGBT in community | 114 LB women (n = 212 total) | Convenience sample, including from pubs and clubs | Self-report lesbian/gay women or bisexual women | Fertility, screening (most results not split by gender) | Grey literature report. Commissioned by NHS Bradford and Airedale |
| McDermott et al. 2016 | Survey and interviews | LGBT people in the community aged 16–25 years who had experienced self-harm or suicidal feelings, and mental health services staff | Survey 336 women (n = 789 total), interviews number of women unclear (n = 29 total) | LGBT organisations and social networks, LGBT mental health organisations | Self-report LGB or queer | Experiences of mental health services | Grey literature, funded by Department of Health Policy Research Programme |
| Price 2010 (and Price 2012) | Semi-structured interviews | LGB carers of people with dementia | 11 SMW (n = 21 total) | Through Alzheimers’ Society then online fora, conference, advertising, word of mouth | Unclear | Experiences of dementia services | Fully published, funding unclear |
| River 2011 | Survey (open and closed questions) | LGBT people aged over 50 | 144 SMW n = 283 total) | Through Polari Group mailing list, specialist websites, emails to community lists and social and campaigning groups in London | Self-report LGB | Experiences of GP services | Grey literature, funded by Age Concern England |
| Urwin and Whittaker 2016 | English General Practice Patient Survey 20012/14 | Women in community attending GPs | 1,138,653 women of which 0.6% lesbian, 0.4% bisexual. 91.9% heterosexual (n = 2,807,320 total) | Through GP surgeries | Self-report LGB using ONS categories | GP practice use | Fully published, not funded |
| Westwood 2016 (and Westwood 2016b) | Semi-structured interviews | Older LGB in community or sheltered housing | 36 SMW (n = 60 total) | Convenience sample via online adverts social networks, word of mouth, | Self-report various self-labels | Housing and residential care provision, concerns around dementia care | Fully published, funding unclear |
| Willis et al. 2011 | Two focus groups and semi-structured interviews | Care stakeholders including carers | 2 lesbian carers (n = 10 total) | Multiple channels including electronic fliers, Facebook, LGBT organisations | Self-report | Carers’ experiences | Fully published, University of Birmingham seedcorn funding |
| Study | Lesbian | Bisexual | Mixed | Heterosexual/ Comparator | Statistical Significance | Notes | |
|---|---|---|---|---|---|---|---|
| Balding 2014 | Visited GP within previous 6 months | NG | NG | 84% (77/92) | 76% (146/1916) | NG | Comparator is Cambridgeshire girls |
| Felt uncomfortable or very uncomfortable talking to doctor or other surgery staff on last visit | NG | NG | 34% (31/92) | 26% (50/1916) | NG | ||
| Elliott et al. 2014 | Trust and confidence in doctor = not at all | 5.3% (95% CI 4.7–5.9) | 5.3% (95% CI 4.6–6.0) | NG | 3.9% (95% CI 3.8–3.9) | p < 0.001 both | Precise numbers for each question varied, numbers by sexual orientation not given. Adjusted percentages controlled for age, race/ethnicity, self-rated health, deprivation quintiles |
| Doctor communication any item = poor or very poor | 11.7% (95% CI 10.8–12.5) | 12.8% (95% CI 11.9–13.7) | NG | 9.3% (95% CI 9.2–9.4) | p < 0.001 both | ||
| Nurse communication any item = poor or very poor | 7.8% (95% CI 7.1–8.4) | 6.7% (95% CI 5.9–7.5) | NG | 4.5% (95% CI 4.5–4.6) | p < 0.001 both | ||
| Overall satisfaction = fairly or very dissatisfied | 4.9% (95% CI 4.3–5.5) | 4.2% (95% CI 3.6–4.8) | NG | 3.9% (95% CI 3.8–3.9) | p < 0.001 and p = 0.31 | ||
| GEO 2018 | Did not discuss or disclose sexual orientation because afraid of a negative reaction | NG | NG | 15.6% (cis) | NG | NG | Results given separately for cis and trans women. No heterosexual comparator for cis SMW. Nine percent of trans women were heterosexual, but results not given separately for SMW transwomen (or versus heterosexual transwomen) |
| Did not discuss or disclose sexual orientation because had a bad experience in past | NG | NG | 5.8% (cis) | NG | NG | ||
| Did not discuss or disclose sexual orientation because afraid of being outed | NG | NG | 5.4% (cis) | NG | NG | ||
| Unsuccessful in accessing mental health services | NG | NG | 9% (cis) | NG | NG | ||
| Rated access to mental health services ‘not at all easy’ | NG | NG | 27.4% (cis) | NG | NG | ||
| Experience of mental health services mainly or completely negative | NG | NG | 22.2% (cis) | NG | NG | ||
| Accessing sexual health services not easy | 31% | NG | NG | NG | NG | ||
| Had to wait too long to access sexual health services | NG | NG | 12.1% (cis) | NG | NG | ||
| Was not able to go at a convenient time | NG | NG | 11.5% (cis) | NG | NG | ||
| Worried, anxious or embarrassed about going to sexual health services | NG | NG | 8.9% (cis) | NG | NG | ||
| Sexual health services were not close | NG | NG | 7.1% (cis) | NG | NG | ||
| Did not know where to go to access sexual health services | NG | NG | 5.9% (cis) | NG | NG | ||
| GP was not supportive | NG | NG | 4.2% (cis) | NG | NG | ||
| GP did not know where to refer for sexual health services | NG | NG | 2.3% (cis) | NG | NG | ||
| Experience of sexual health services mainly or completely negative | NG | NG | 17.3% (cis) | NG | NG | ||
| Guasp 2011 | Experienced discrimination, hostility or poor treatment because of their sexual orientation when using GP services | NG | NG | 17% | NG | NG | Numbers unclear, 40% of these incidents within previous 5 years |
| Been excluded from a consultation or decision-making process with regard to their partner’s health or care needs | NG | NG | 14% | 6% | NG | Numbers unclear | |
| Hidden the existence of a partner when accessing services like health, housing and social care | NG | NG | 12% | <1% | NG | Numbers unclear | |
| Humphreys et al. 2016 | Negative experience of GP/Primary care | NG | NG | 47% (24/51) | NG | NG | Denominator numbers unclear |
| Negative experience of hospital | NG | NG | 66% (18/27) | NG | NG | ||
| Negative experience in a mental health setting | NG | NG | 66% (4/6) | NG | NG | ||
| Negative experience in sexual health clinic | NG | NG | 57% (8/14) | NG | NG | ||
| Light and Ormandy 2011 | Refused or discouraged from having a cervical screen by a health professional because of their sexual orientation | NG | NG | 14% (70/500) | NG | NG | |
| Macredie 2010 | Refused a cervical screen or advised it was not necessary | NG | NG | 6% (7/114) | NG | NG | |
| Found screening staff to be helpful but lacking in knowledge of lesbian and bisexual women | NG | NG | 57% (33/62) | NG | NG | Of those screened | |
| Found screening staff to be unhelpful and lacking in knowledge of lesbian and bisexual women | NG | NG | 12% (7/62) | NG | NG | ||
| River 2011 | Bad experiences of General Practice | NG | NG | 31% (45/144) | NG | NG | |
| Urwin and Whittaker 2016 | Odds ratio of visiting a family practitioner for any reason | 0.803 (0.755–0.854) | 0.887 (0.817–0.963) | NG | Referent | p < 0.001 and p = 0.004 | Adjusted for patient and GP practice characteristics |
| No | Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Almack et al. 2010 | Y | Y | Y | Y | Y | CT | CT | Y | Y | Y |
| 2 | Bristowe et al. 2018 | Y | Y | Y | Y | Y | CT | CT | Y | Y | Y |
| 3 | Carter et al. 2013 | Y | Y | Y | Y | Y | CT | CT | CT | Y | Y |
| 4 | Cherguit et al. 2012 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| 5 | Evans and Barker 2010 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| 6 | Fenge 2014 | Y | Y | Y | Y | Y | N | Y | Y | Y | Y |
| 7 | Fish 2010 | Y | Y | Y | Y | Y | CT | Y | N | Y | Y |
| 8 | Fish and Bewley 2010 | Y | Y | Y | Y | Y | CT | Y | Y | Y | Y |
| 9 | Fish and Williamson 2016 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| 10 | Formby 2011 | Y | Y | Y | Y | Y | N | Y | CT | Y | Y |
| 11 | Guasp 2011 | Y | Y | Y | Y | Y | N | Y | CT | Y | Y |
| 12 | Humphreys et al. 2016 | Y | Y | CT | Y | Y | CT | CT | N | Y | Y |
| 13 | Ingham et al. 2016 | Y | Y | Y | Y | Y | Y | CT | Y | Y | Y |
| 14 | Knocker 2012 | Y | Y | Y | CT | Y | N | CT | N | Y | Y |
| 15 | Lee et al. 2011 | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y |
| 16 | Light and Ormandy 2011 | Y | Y | Y | Y | Y | CT | Y | Y | Y | Y |
| 17 | Macredie 2010 | Y | Y | Y | CT | Y | CT | CT | N | Y | N |
| 18 | McDermott et al. 2016 | Y | Y | Y | Y | Y | CT | Y | Y | Y | Y |
| 19 | Price 2015 | Y | Y | Y | Y | Y | CT | Y | Y | Y | Y |
| 20 | River 2011 | Y | Y | Y | Y | Y | N | Y | CT | Y | CT |
| 21 | Westwood 2016 | Y | Y | Y | Y | Y | CT | Y | CT | Y | Y |
| 22 | Willis et al. 2011 | Y | Y | Y | Y | Y | CT | CT | Y | Y | Y |
| Study | 1 | 2 | 3 | 4 | 5a | 5b | 6a | 6b | 9 | 10 | 11 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Balding 2014 | y | y | y | ct | ct | ct | n/a | n/a | y | y | n/a |
| 2 | Elliott et al. 2014 | y | y | y | y | y | y | n/a | n/a | y | y | y |
| 3 | GEO 2018 | y | y | y | y | y | ct | n/a | n/a | y | y | y |
| 4 | Guasp 2011 | y | y | y | y | ct | n | n/a | n/a | y | y | y |
| 5 | Humphreys et al. 2016 | y | ct | ct | y | ct | n | n/a | n/a | n | ct | y |
| 6 | Light and Ormandy 2011 | y | y | ct | y | ct | n | n/a | n/a | y | y | y |
| 7 | Macredie 2010 | y | ct | ct | y | ct | n | n/a | n/a | y | y | y |
| 8 | River 2011 | y | y | ct | y | ct | n | n/a | n/a | y | y | y |
| 9 | Urwin and Whittaker 2016 | y | y | y | y | y | y | n/a | n/a | y | y | y |
| Summary of Review Findings | Qualitative Studies Contributing* | Methodological Limitations | Relevance | Coherence | Adequacy | Assessment of Confidence in the Evidence | Explanation of CERQual Assessment | |
|---|---|---|---|---|---|---|---|---|
| 1 | Unhelpful health ambience.Women reported that the environment did not include them | 3,5–7, 10,12,14,17,19,20 | Minor methodological concerns due to sample size of some studies and some data coding and analysis undertaken by only one researcher | Very minor concerns. Some studies are extremely local, but the studies together present a coherent picture | Very minor concerns as data consistent within and across studies | Very minor concerns despite low number of participants in some studies. Studies together provide rich data | High | This finding was graded as high as together these 10 studies present a coherent picture of women’s experience. Larger studies confirm findings of smaller studies. Rich data supports findings. |
| 2 | Assumed Heterosexuality /Heteronormativity | 2,4– 12,17,20 | Very minor methodological considerations due to lack of clarity concerning researcher role and potential bias in design and analysis of most studies. | Very minor concerns. Some studies very local or in big cities, | Very minor concerns. Findings are consistent within and across studies | Minor concerns due to small sample size of some studies. Larger studies provide very rich data and confirm findings of smaller studies. | High | This finding was graded as high despite very minor concerns in a minority of studies as together these studies provide rich data from a wide variety of settings. The 12 studies included provide a consistent picture regardless of service setting and service user group |
| 3 | Being Out or not | 1,3–14,16,19,20 | Very minor methodological considerations due to lack of clarity concerning researcher role and potential bias in design and analysis of most studies. | Very minor concerns. All demonstrate relevance to overall topic | Very minor concerns. Consistency across studies demonstrated. Data support findings | Studies together provide rich data across a variety of health and social care settings | High | This finding was graded as high despite some studies having a small number of participants as there was consistency of findings regardless of setting, geographical location and service user group. Sixteen studies contributed to this finding and rich data were evidenced |
| 4 | Responses to Being Out | 4,5,7–9,12,15–17,22 | Very minor methodological considerations due to lack of clarity concerning researcher role and potential bias in design and analysis of most studies. | Very minor concerns. All demonstrate relevance to overall topic | Very minor concerns. Data consistent within and across studies | Minor concerns due to sample size in some studies which offered little data about women’s experience, | High | This finding was graded as high despite minor concerns as ten studies contributed to this theme and larger studies provided consistent, rich data which supported the findings of smaller studies |
| 5 | Ignorance | 3,5,8,10,12,15–17,22 | Very minor methodological considerations due to lack of clarity concerning researcher role and potential bias in design and analysis of most studies. | Very minor concerns. All demonstrate relevance to overall topic | Very minor concerns. Data consistent within and across studies | Minor concerns as some studies were aiming to improve particular services. | High | This finding was graded as high as nine studies contributing to this theme provided rich data to support findings. Consistency and relevance across the studies assures the findings. |
| 6 | Impact on SMW | 2,3,7,10–13,15,16,20 | Very minor methodological considerations due to lack of clarity concerning researcher role and potential bias in design and analysis of most studies. | Minor concerns. All demonstrate relevance to overall topic | Very minor concerns. Data consistent within and across studies | Moderate concerns as half of these studies were categorised as ‘grey’ literature and half had small numbers of participants | Moderate-High | This finding was graded as moderate to high as a half of the studies were categorised as grey literature and half had relatively small numbers of participants. Despite this, data were consistent across studies. |
| 7. | Challenging/ Complaining | 4,7–9,12,16,20 | Very minor methodological considerations due to lack of clarity concerning researcher role and potential bias in design and analysis of most studies. | Minor concerns | Very minor concerns. Data consistent within and across studies | Minor concerns, as this theme was not the focus of studies in most cases and the data were moderately rich | Moderate | This finding was graded as moderate. The data were consistent but lacked richness. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meads, C.; Hunt, R.; Martin, A.; Varney, J. A Systematic Review of Sexual Minority Women’s Experiences of Health Care in the UK. Int. J. Environ. Res. Public Health 2019, 16, 3032. https://doi.org/10.3390/ijerph16173032
Meads C, Hunt R, Martin A, Varney J. A Systematic Review of Sexual Minority Women’s Experiences of Health Care in the UK. International Journal of Environmental Research and Public Health. 2019; 16(17):3032. https://doi.org/10.3390/ijerph16173032
Chicago/Turabian StyleMeads, Catherine, Ros Hunt, Adam Martin, and Justin Varney. 2019. "A Systematic Review of Sexual Minority Women’s Experiences of Health Care in the UK" International Journal of Environmental Research and Public Health 16, no. 17: 3032. https://doi.org/10.3390/ijerph16173032
APA StyleMeads, C., Hunt, R., Martin, A., & Varney, J. (2019). A Systematic Review of Sexual Minority Women’s Experiences of Health Care in the UK. International Journal of Environmental Research and Public Health, 16(17), 3032. https://doi.org/10.3390/ijerph16173032